Identifying Progressive CKD from Primary Care Records – a Study Protocol
An absract published in the British Renal Society 2017 (BRS2017)
Figure a
Background
One of the key challenges in managing CKD patients is to identify those who are progressive (worsening eGFR) from those who are non-progressive or may even have underlying improvement in their CKD. To this end, we have developed an algorithm capable of identify progressive from non-progressive CKD based on observed historical eGFR trends.
Methods - Clinical codes.
We identified 5-Byte Read Codes from the Royal College of General Practioners (RCGP) Research and Surveillance Centre (RSC) for a range of known factors, including codes related to signs and symptoms (), laboratory measurements () and treatments () for CKD as well as its associated co-morbidities or risk factors (r) such as diabetes, cardiovascular disease and kidney-related diseases. For each risk factor, and are systematically identified, leading to a range of plausible phenotype variables for explaining a rapid decline in eGFR (See our Bayesian Justification accompanying poster). Algorithm. We have developed our own regression algorithm – called the broken-stick model – capable of estimating the rate change of eGFR by using a ‘Bayesian’ sliding window of three years in order to provide a stable estimate of the annual rate change of eGFR, while still being sensitive to underlying genuine patterns. The global eGFR slope (annual rate change) of a patient is defined as the average eGFR slope over the patient’s entire history.
Patient inclusion/exclusion criteria
All patients with eGFR measurements were included. Patients with an acute kidney injury episode or hereditary kidney diseases were excluded. Additionally, patients without consistent eGFR trends, defined as having a standard deviation of the eGFR slope of 2 units per year, were excluded.
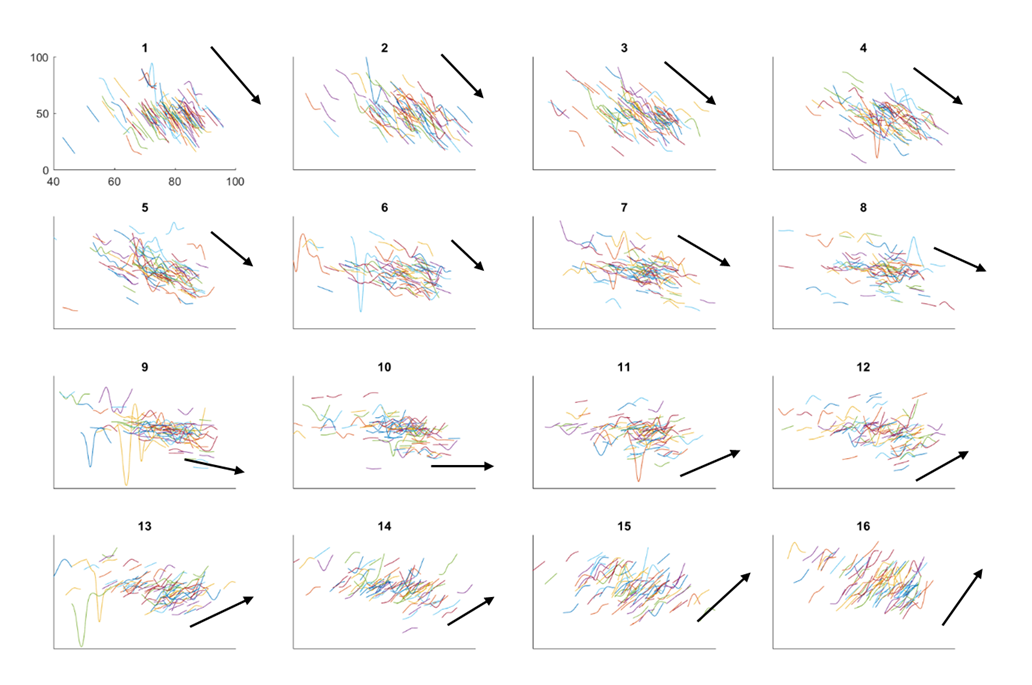
Initial descriptive observations
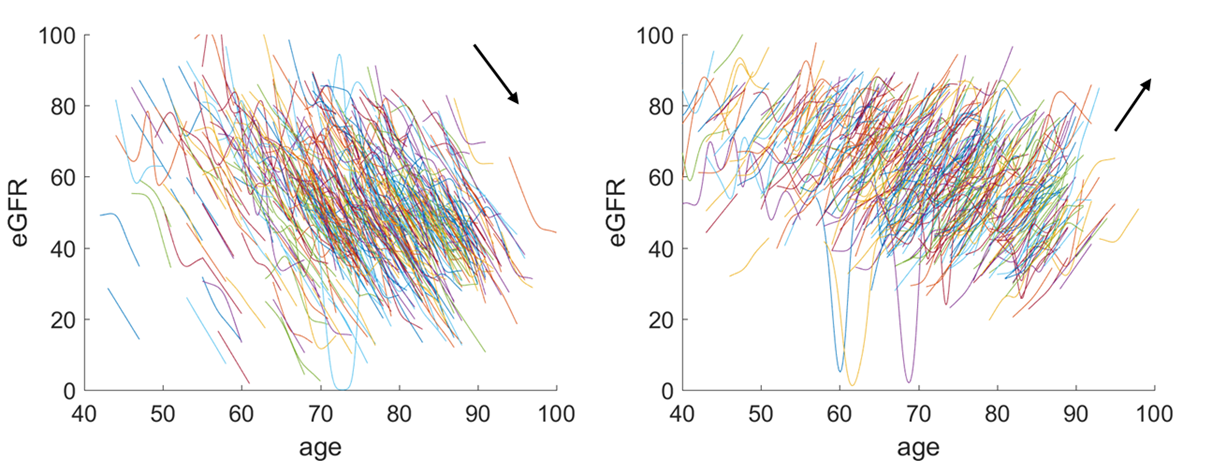
The longitudinal observational data was divided into equal groups of approximately 600 patients. In 9 out of 16 groups (see figure a) we found that there was a deterioration in eGFR, one group was equivocal and six groups showed improvement. Figure b below compares the eGFR trends of the first group with the last group, group 16. It is clear that the first group of patients have very drastic decline in CKD. Understanding the factors that contributing to or even distinguish them from the other groups is the important step.
Figure b
Conclusions
A systematic cohort-based retrospective observational study, based on routinely collected primary care data coupled with advanced machine learning algorithms, could improve our understanding of the nature of the rapid progression of CKD in some groups (group 1) of patients in contrast to those (group 16) that show an improvement in eGFR.
What’s next?
Download the abstract here and the poster here.
Cite this blog post
Bibtex
@misc{ poh_2018_01_13_BRS2017-progressive-ckd,
author = {Norman Poh},
title = { Identifying Progressive CKD from Primary Care Records – a Study Protocol },
howpublished = {\url{ http://normanpoh.github.com/blog/2018/01/13/BRS2017-progressive-ckd.html},
note = "Accessed: ___TODAY___"
}